")
ACL Injuries: The good, the bad, the ugly: A preventative approachAnnemarie Alf, PT, DPT, CSCS, SFMA If you missed the first two chapters of Annem
ACL Injuries: The good, the bad, the ugly: A preventative approach
Annemarie Alf, PT, DPT, CSCS, SFMA
If you missed the first two chapters of Annemarie Alf’s ACL series, be sure to check them out here!
One of the most common and yet most dreaded injuries a soccer player can endure, is to hear that you’ve torn your ACL- anterior cruciate ligament. The ACL is a ligament in the center of the knee joint that prevents the tibia- lower leg bone from sliding anterior or forward on the femur bone- upper leg bone.
This week we will look at what to expect if you do need to have your ACL repaired and what the post- rehab and return to sport should look like.
Types of ACL repair grafts: 2 main types
The most commonly used are the autografts (patellar bone & hamstring) and sometimes the allografts- taken from a piece of cadaver tissue. There is no consensus in the literature as to which provides the most stability for the knee. Each of these choices has advantages and disadvantages.
Patellar Tendon- my personal and professional preference
When a patellar tendon graft is taken, the central 1/3 of the patellar tendon is removed (about 9 or 10 mm) along with a block of bone at the sites of attachment on the kneecap and tibia.
Advantages of a Patellar Tendon Graft for the ACL: Closely resembles the structures to be replaced. The length of the patellar tendon is close to that of the ACL and the bone ends of the graft can be placed into the bony attachment points of the ACL. Early bone to bone healing is around 6 weeks. Bone to bone healing is considered to be stronger than soft tissue to bone healing as with a hamstring graft.
Disadvantages for Patellar Tendon Graft: More likely to sustain Patellar Tendinitis and anterior knee pain; Patellofemoral joint tightness with late chondromalacia; Loss of range of motion

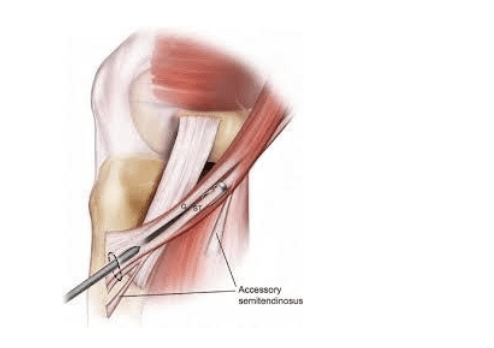
Hamstring Graft: With the improvement in the technique of the preparation of the multiple bundle graft, this graft choice has become more popular by many surgeons.
Advantages: No risk of anterior knee pain as with the patellar tendon; smaller incision; Pain in the immediate post-operative period is less.
Disadvantages: Graft fixation to bone requires additional ‘hardware’ i.e. screws, endobutton. Graft healing of soft tissue to bone takes longer to heal, 10-12 weeks.
*** Patients may struggle to regain full strength of the hamstrings from which the donor was taken.
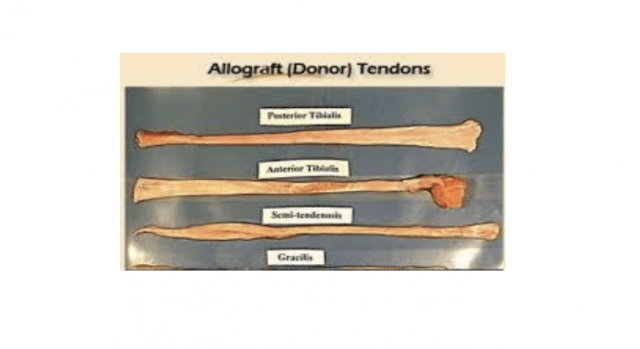
Allograft (Donor Tissue)- aka Cadaver Graft
Allograft is most commonly used in lower demand patients, or patients who are undergoing revision ACL surgery. Biomechanical studies show that allograft (donor tissue from a cadaver) is not as strong as a patient’s own tissue (autograft). For many patients, however, the strength of the reconstructed ACL using an allograft is sufficient for their demands. Therefore, this may be an excellent option for patients not planning to participate in high demand sports such as football, basketball, etc.
Advantages of an allograft: Decreased operation time/ No need to remove other tissue to use for the graft/ Smaller incisions/ Less post-operative pain
Disadvantages: Risk of body rejecting cadaver graft; Graft preparation decreases the strength of the tissue; Longer graft to bone incorporation time.
Ultimately, if you find yourself in the situation of needing to have you ACL repaired the decision is up to you and what you feel is the best option for you. This should be a discussion between you and your surgeon and you should weigh all the options.
The 3 Phases of rehab after ACL repair
Phase 1: Immediate rehab following ACL repair is the MOST important component.
Find a Physical Therapist that specializes in return to sport rehab and address the WHOLE athlete.
- Restore Range of Motion early and regain Quad control immediately
- Weight bearing and return to normal gait as soon as possible
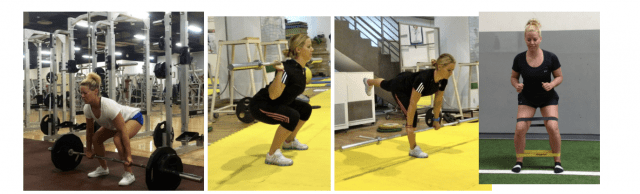
Phase 2: Strength Focus
- Regaining quad and hamstring strength to at least 85% of non- surgical leg.
Focus should be primarily on CKC- closed kinetic chain activities such as squats, deadlifts.
- A progression and emphasis into single leg strength – lunges, step downs, single leg RDLs to name a few for the foundational strength phase.
Phase 3: Return to Sport
- Running can typically begin in the 3-4 month post- surgical window BUT this is very dependent on current strength, range of motion and hip control.
- Focus should be on sport- specific demands- overall movement patterns, jumping and landing technique, change of direction and speed work.
- Every sport has its demands that MUST be taken in consideration, when rehabbing to return an athlete to sport.
- Return to sport windows can be anywhere between 6-9-12 months.