")
This Week from Olympus ACL Injuries: The good, the bad, the ugly: A preventative approach, by Annemarie Alf, PT, DPT, CSCS, SFM One of the most
This Week from Olympus
ACL Injuries: The good, the bad, the ugly: A preventative approach, by Annemarie Alf, PT, DPT, CSCS, SFM
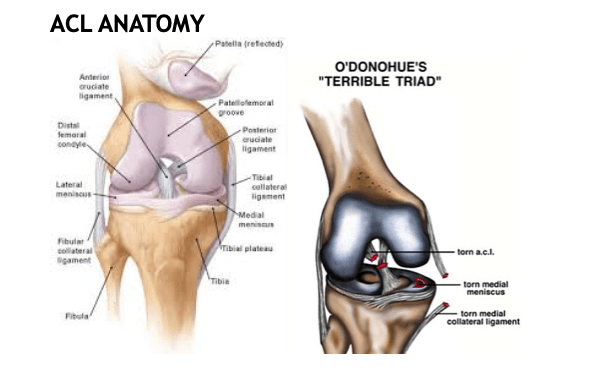
One of the most common and yet most dreaded injuries a soccer player can endure, is to hear that you’ve torn your ACL- anterior cruciate ligament. The ACL is a ligament in the center of the knee joint that prevents the tibia- lower leg bone from sliding anterior or forward on the femur bone- upper leg bone.
This week we will look at common causes and reasons for ACL tears, BUT stay tuned for next week where we discuss more specifically HOW we can reduce these injuries and then week 3, what to expect if you do need to have your ACL repaired and what the post- rehab and return to sport should look like.
What’s worse than just tearing your ACL alone, is sustaining the ‘terrible triad’: which is tearing the ACL, medial meniscus and MCL- medial collateral ligament all together.
We are going to go thru a brief overview of how ACL injury statistics, some of their mechanisms and risk factors, but then most importantly discussing what injury reduction programs should look like and include.
Statistics for ACL Injuries
Unfortunately, female athletes competing in sports that include jumping and cutting demonstrate a 4-10x higher incidence of knee injury than do male athletes in the same sports.
Mechanisms of ACL Injuries: Contact vs Non- Contact Injuries
Two thirds of all ACL injuries are non-contact injuries and the three major ways that these injuries occur:
1. Planting and Cutting
2. Straight knee landing
3. One step stop landing with a hyperextended knee
All non- contact injuries are correlated with knee torsion, deceleration, rapid change in direction. These are the types of ACL injuries that can be reduced via proper training programs.
Only 1/3 of the ACL knee injuries are from a contact injury.
Risk factors that may CONTRIBUTE TO ACL tears:
- EXTRINSIC FACTORS (happening outside of our body):
- Meteorological/ Weather conditions- think playing on wet surfaces (Orchard et al). We can’t necessarily avoid this, but we can be more aware of our body positioning and angles.
- Type of surface- there has been some research showing that turf fields have a higher risk of injury. (Myers MC, Barnhill BS)
- Type of footwear- not wearing the right type of footwear for the type of surface you are playing on. (Lambon et al)

- INTRINSIC FACTORS (factors which are within the body. It is also the physical aspect of the athlete’s body that can cause injury.)
For the most part we can control or influence these initial 5 intrinsic factors with implementation of proper strengthening and neuromuscular control programs.
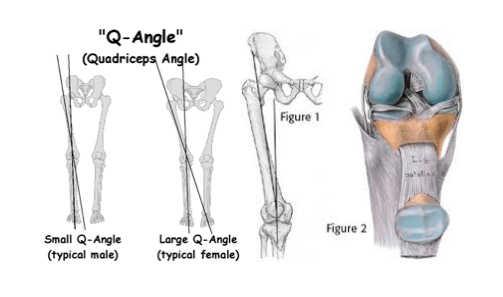
- Q angle- (Shambaugh et al)
- Knee valgus- (Ford et al; Hewett et al) Over 22.5 Nm indicates high risk (Hewett et al)
- Foot pronation- (Allan and Glascoe; Woodford-Rogers et al)
- Excessive hip adduction due to weak hip stabilizers- (C. Powers)
- Body mass index- (Brown et al; Knapik et al)
1, Q Angle: The Q angle is measured by creating two intersecting lines: one from the center of the patella (kneecap) to the anterior superior iliac spine of the pelvis; the other from the patella to the tibial tubercle. There is research to support, that the larger the Q angle, the more prone an athlete might be to a knee injury. However, we would argue that this athlete needs to just be more diligent about following an ACL injury reduction program.
2, Knee Valgus/ Foot Pronation and Hip Adduction: it is very common and likely to see these 3 factors occur together.
Knee control from the hip stabilizers, posterior chain muscles and foot intrinsics are arguably the most important factors in the reduction of ACL injuries.


Additional Rick Factors
- Notch Size/ACL Size (Souryal and Freeman and Shelbourne and Kerr)-
- Hormones (Shultz et al; Wojtys et al; Slauterbeck et al)
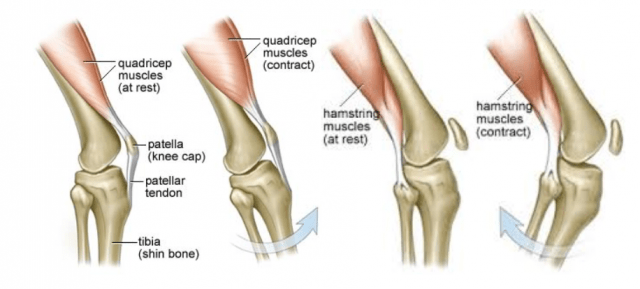
- Altered muscle activation patterns (Hutson and Wojtys; Malinzak et al) Quadriceps dominant contraction
- Inadequate muscle stiffness (Kibler and Livingston; Granata et al)
- Abnormal loading of the knee due to unsuccessful dynamic postural adjustments (Chris Powers; Griffin et al.)

Neuromuscular Performance Characteristics in Elite Female Athletes
The American Journal of Sports Medicine Vol Huston et al. 24:427-434
- The purpose of the research was to identify possible predisposing neuromuscular factors for knee injuries in female athletes. These factors include anterior knee laxity, lower extremity muscle strength, endurance, muscle reaction time, and muscle recruitment order in response to anterior tibial translation.
ACL RESEARCH RESULTS (Huston et al. 24 )
- Female athletes demonstrated more anterior tibial laxity than their male counterparts and significantly less muscle strength and endurance
- Compared with the male athletes the female athletes took significantly longer to generate maximum hamstring muscle torque during isokinetic testing
- Female athletes relied more on their quadriceps muscles in response to anterior tibial translation; the three other test groups relied more on their hamstring muscles for initial knee stabilization
- So what does this mean?
STAY TUNED FOR NEXT WEEKS ACL INJURIES – HOW TO DECREASE RISK!
**Contributing factors that CAN be changed or trained (Arendt et al and Griffin et al)
- Joint proprioception
- Neuromuscular recruitment and muscle imbalances (quad-hamstring ratio)
- Muscle strength (both eccentric and concentric) and flexibility
- Joint posture and alignment
- Resistance to fatigue